News
National GMSA Transformation Project: Lynch Syndrome

Update
National GMSA Transformation Project: Lynch Syndrome
Delivery of a comprehensive service for the detection of Lynch syndrome
December 2, 2022
Delivery of a comprehensive service for the detection of Lynch syndrome
December 2, 2022
On this page you will find;
Lynch Syndrome (LS) is an inherited condition which results in an increased risk of certain cancer types. The main concerns are colorectal and endometrial cancer. There is also an increased risk to other cancers, but they are less frequent. People with LS have up to an 80% risk of developing colorectal cancer in their lifetime and, in women, up to a 60% risk of developing endometrial cancer.
In total LS affects approximately 1 in 350 to 1 in 400 people, with 200,000-300,000 people likely to have this condition in the UK. However, it is estimated that only 5% of people with LS in the UK have been diagnosed.
Identifying people with LS provides the opportunity to detect cancers at an earlier stage through enrolment into screening programmes, and prevent cancers through risk reduction techniques including colonoscopy, prophylactic surgery and chemoprophylaxis with aspirin.
A diagnosis of LS can also influence management plans for people who develop cancer, including impacting the surgical approaches chosen and the use of specific immunotherapy and chemotherapy treatments, and may impact access to emerging therapies.
In addition to preventing cancer and maintaining the health and quality of life of patients and families with LS, there is consistent evidence of the cost-effectiveness of a structured diagnostic pathway in patients with LS following a diagnosis of cancer, linked to cascade testing in families.
Led by the North Thames and South East GMSAs, the NHS GMS National Lynch Syndrome project is working to improve the identification and management of Lynch Syndrome, bridging the gap in testing and diagnosis of Lynch Syndrome and supporting the early detection of cancer and access to personalised care. The project will initially focus on colorectal and endometrial cancer patients and over time the programme will aim to extend LS screening across relevant tumour types.
The GMSAs are collaborating closely with the Cancer Alliances, National Disease Registry Service (NDRS), National Cancer Registration and Analysis Service (NCRAS), and the NHS England Cancer Programme to:
Nationally, over 200 MDT Lynch Champions have been appointed to be responsible for Lynch testing pathways across their geographies. These Champions are supported by a network of Regional Lynch Nurses and Clinical Project Leads and are a central member of the Regional Expert Networks that are being established.
A national forum with regional project teams, MDT Champions, Cancer Alliance representatives and other key stakeholders convenes on a regular basis to facilitate discussion of common issues and shared solutions.
The national project leadership team have collaborated with the NDRS to deliver a Lynch data dashboard on CancerStats2 (to request access follow this instructions), linking national dataset to provide regional and Provider level performance monitoring at each stage of the Lynch testing pathway, including MMR, BRAF and MLH and germline genetic testing. The current full complement of NDRS data includes all patients diagnosed in 2019 with endometrial or colorectal cancers. Although this baseline data shows low access to testing, more recent self-reported data collected by this project via a national survey indicates that this will have increased over the past few years. The NDRS plan to provide more contemporary data for Lynch Syndrome testing and GMSAs are working with GLHs to access other datasets and MDTs are completing local audits to continue monitoring geographical variation and measure impact of project activities on equity of access to testing and appropriate interventions.
Colonoscopy surveillance for people living with Lynch syndrome will be delivered by the National Bowel Cancer Screening Programme (NBCSP) from April 2023. Training for BCSP staff is available. If you work for the BCSP you can register for the live online training here.
Clinical genetics departments will ensure that anyone with a diagnosis of Lynch syndrome is registered in the NBSC. Even if you are consenting patients for genetic testing for Lynch syndrome, you will always refer patients to your linked clinical genetics department for a review and cascade testing. This will ensure that all patients are enrolled into the program, so cancer MDTs will not be expected to do this.
Clinical genetics departments will securely provide the National Disease Registration Service (NDRS) with details of people diagnosed with Lynch syndrome. NDRS then provide the screening programme with a list of people who need screening. This ensures people diagnosed with Lynch syndrome receive high quality care.
Regional Lynch syndrome network Launch: February 2023
Online training modules for Colorectal Cancer MDTs
Online training modules for Endometrial Cancer MDTs
Online training modules for Pathologists & Supporting documents with guidance on reporting
How to order a test:
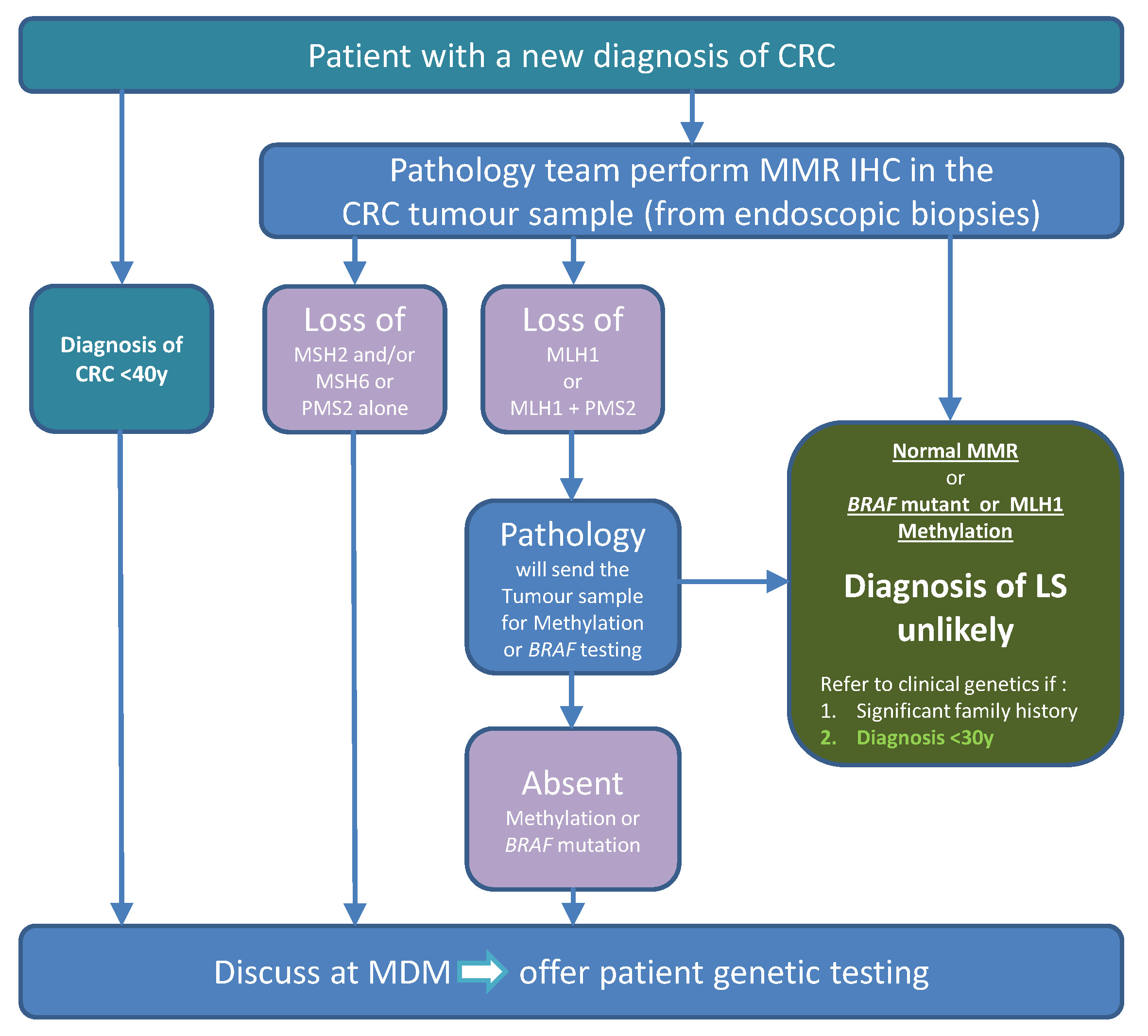
1. Region specific testing pathway/algorithm:
3. Region specific supporting documents:
Dr Kevin Monahan, North Thames GMSA; Consultant Gastroenterologist, Lynch Syndrome and Family Cancer Clinic, St Mark’s Hospital: k.monahan@nhs.net
Dr Adam Shaw, South East GMSA, Consultant in Clinical Genetics Guy’s and St Thomas’ NHS Foundation Trust: Adam.Shaw@gstt.nhs.uk
Laura Monje-Garcia, North Thames GMSA, Nurse Practitioner and Clinical Research Fellow, St Mark’s centre for familial intestinal cancer: laura.monje-garcia@nhs.net
Regional Lynch syndrome lead: Dr Kevin Monahan K.Monahan@nhs.net
Regional Lynch syndrome nurse: Anna Koziel Anna.Koziel@nhs.net
National lead Nurse for the Lynch syndrome project: Laura Monje-Garcia Laura.Monje-Garcia@nhs.net
Regional Expert Centre for North Thames Region
The St Mark’s Centre for Familial Intestinal Cancer
Polyposis, Lynch and family cancer
St Mark’s Hospital, Central Middlesex Hospital Site, Acton Lane, Park Royal NW10 7NS
Tel: 020 8453 2656 | Email: LNWH-tr.SMCFIC@nhs.net
Website: www.polyposisandlynch.com
For the South East GMSA region you can contact:
Regional Lynch syndrome lead: Dr Adam Shaw Adam.Shaw@gstt.nhs.uk
Regional Lynch syndrome nurse: Aela.Limbu@gstt.nhs.uk
Region specific website & resources: https://southeastgenomics.nhs.uk/lynch-syndrome/
For the South West GMSA region you can contact:
Regional Lynch syndrome lead: Frank McDermott f.mcdermott@nhs.net
Regional Lynch syndrome nurse: Sarah.John@nbt.nhs.uk & Siobhan.john@nhs.net
For the North East & Yorkshire GMSA region you can contact:
Regional Lynch syndrome lead: Dr Jackie Cook jackie.cook8@nhs.net and Dr Sally Lane sallylane@nhs.net
Regional Lynch syndrome nurse: Amy.sanderson5@nhs.net; K.westaway@nhs.net & Rebecca.foster26@nhs.net
Region specific website & resources: https://ney-genomics.org.uk/our-work/lynch-syndrome-improving-patient-outcomes/
North West GMSA region you can contact:
Regional Lynch syndrome lead: Fiona Lalloo Fiona.Lalloo@mft.nhs.uk
Regional Lynch syndrome nurse: Miranda.Darbyshire@elht.nhs.net
Region specific website & resources: https://www.nw-gmsa.nhs.uk/education-and-research/et-resources/lynch-syndrome-genetic-testing-pathway
Central & South GMSA region you can contact:
Clinical Medical Lead: David Church david.church@well.ox.ac.uk
Deputy Medical Lead: Alaa El-Ghobashy alaaelghobashy@nhs.net
Regional Lynch syndrome nurse: Felicity Blair Felicity.Blair@uhb.nhs.uk
Programme Manager: Lisa Dew lisa.dew@uhb.nhs.uk
Project Manager: Sarah Hewett Sarah.Hewett@uhb.nhs.uk
Region specific website & resources: https://centralsouthgenomics.nhs.uk/transformation-projects-patients/lynch-syndrome/
East GMSA region you can contact:
Regional Lynch syndrome lead: Ruth Armstrong ruth.armstrong@addenbrookes.nhs.uk
Region specific website & resources: https://www.eastgenomics.nhs.uk/about-us/genomic-medicine-service-alliance/Transformation_Projects/lynch-syndrome/
National lead nurse for the Lynch syndrome project (based North Thames GMSA region): Laura Monje-Garcia Laura.monje-garcia@nhs.net
Providing expertise & training in gynaecological cancers in Lynch syndrome (based South West GMSA region): Tracie Miles, Associate Director of Nursing & Midwifery Tracie.miles@nhs.net
Providing strategic advice (St Mark’s centre for familial intestinal cancer): Victoria Cuthill, Consultant and Lead Nurse at the St Mark’s Centre for Familial Intestinal Cancer Vcuthill@nhs.net
Lynch syndrome is caused by a genetic change in one of the DNA mismatch repair genes called MLH1, MSH2, MSH6 and PMS2. There is a fifth gene involved called the EPCAM gene because it turns off the neighbouring MSH2 gene. EPCAM alterations are very rare and only account for 6% of Lynch syndrome cases.
The function of DNA mismatch repair genes is to repair errors that may arise in the DNA code, which in turn protect people from developing cancer.
No. Lynch syndrome does not always lead to or cause cancer, but the inherited genetic change that causes Lynch syndrome increases a person’s lifetime risk of developing certain cancer types. The risk of developing cancer from Lynch syndrome depends on the gene affected. The risks associated with variants in PMS2 are much lower than the risks associated with variants in MLH1.
If you believe that your patient may be at risk of developing Lynch syndrome i.e., a strong family history of cancer or family members diagnosed with cancer before the age of 50, then you should recommend referral for a genetic assessment. During the consultation, a family history will be taken and draw a family tree, to assess the risk of an inherited condition in the family.
The national Lynch project’s aim is to test every patient who develops bowel or endometrial cancer for Lynch syndrome.
Patients with diagnosed cancer should have further testing (immunohistochemistry, or IHC, or microsatellite instability MSI) to inform the appropriate diagnostic pathway.
Those with a family history of cancer should be directed to the regional genetics’ units for a family history assessment. Genetic counselling helps patients, and their families better understand their risk for hereditary cancer in order that they can make informed decisions about screening, genetic testing, and follow-on care.
The term ‘mainstreaming’ refers to the shift of genomic testing away from Clinical Genetics to other clinics and specialities. Within the Lynch Syndrome testing pathway, this means healthcare professionals in cancer MDTs becoming directly involved in the consenting of patients for germline genetic testing, the requesting of the test and in communicating the result. A goal of the national GMSA transformation project is to upskill oncology MDTs to provide a mainstream testing service for Lynch Syndrome. This will help ensure all eligible patients receive germline testing without delay and results can effectively inform management.
Join our mailing list to be the first to receive our updates and news!
Newsletter signup

{kind=link}
{kind=link}